
As a cardiothoracic anesthesiologist and intensivist, I routinely place large central lines for resuscitation, vasoactive/inotrope administration, and to facilitate additional monitoring (ie, Swan Ganz catheter). Over the years, I’ve heard “MAC”, “sheath introducer”, “Cordis”, etc., used interchangeably but incorrectly. Let’s break these terms down!
SHEATH INTRODUCER
A “sheath” or “introducer” refers to any line (arterial or venous) that contains a port allowing a proceduralist to “introduce” (hence the name) transvenous pacing wires, Swan Ganz catheters, intravascular ultrasound (IVUS), intra-aortic balloon pumps, single lumen infusion catheters (“SLICs”), etc. The introducer lumen has a one-way diaphragm that prevents back bleeding and can often be capped with an obturator when not in use. The MAC and Cordis are two examples of venous introducers.
The following is a 9 French percutaneous sheath introducer (PSI).
Manufacturer: Arrow/Teleflex
Catheter: percutaneous sheath introducer (PSI)
Lumens: introducer + one infusion port
Compared to the 9 French MAC (see below), the PSI is shorter and, therefore, a better massive resuscitation line due to better flow rates as per Poiseuille’s Law. The big drawback is that it only has one side lumen.
MULTI-LUMEN ACCESS CATHETER (MAC)
Manufacturer: Arrow/Teleflex
Catheter: multi-lumen access catheter (MAC)
Lumens: introducer + two infusion ports (brown distal, white proximal/side)
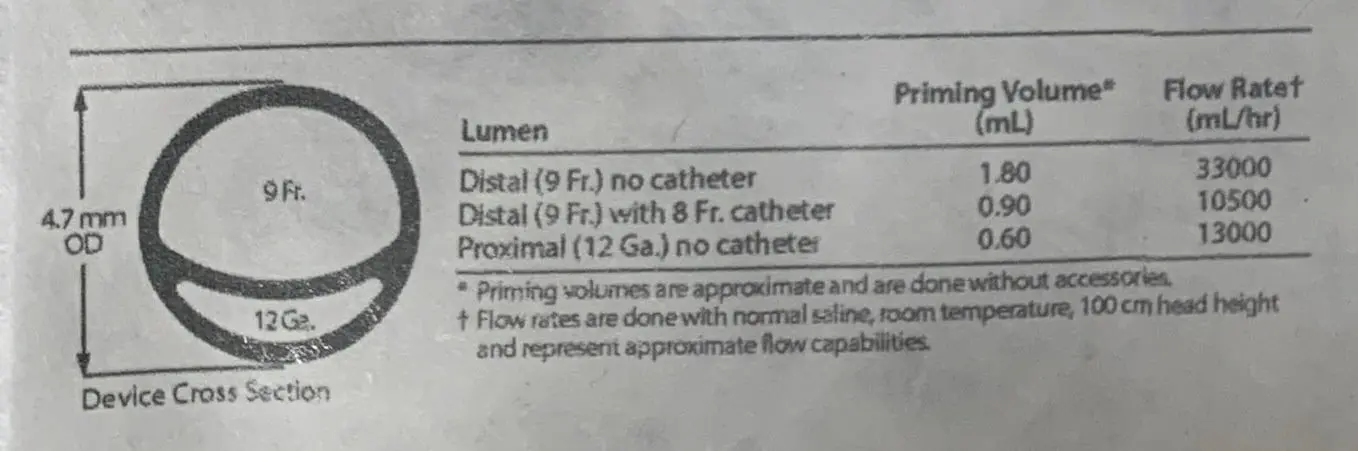
The brown lumen looks larger, so it makes sense that, at baseline, it flows faster than the white lumen. When we look closer at the MAC’s flow rates, notice how if a catheter is inserted into the introducer (e.g., a Swan-Ganz catheter), this steals real estate from the brown lumen and now makes the white lumen the faster-flowing option. In this example, if the introducer is occupied with an 8 French catheter, the distal brown port’s flow is reduced from 33,000 mL/hr to 10,500 mL/hr, making the proximal white port faster (13,000 mL/hr)!
Always read your catheter’s flow rates as this can vary from one version to the next!
Even though this MAC is listed as 9 French in size, that’s only the case at the very distal tip of the catheter. Notice how as you move proximally, it quickly gets larger. Gotta make some room for that second infusion lumen! Based on the device cross-section (4.7 mm outer diameter), the outer diameter is closer to 14 French!
MACs are placed with the dilator inserted through the introducer in one motion rather than sequential steps to facilitate the speed of placement. Once the MAC has been fully inserted, the dilator and guidewire are removed. This style of placement is the same for many introducers.
“CORDIS”
Manufacturer: Cordis (a Cardinal Health Company)
Catheter: AVANTI + Sheath Introducer
Lumens: introducer + one infusion port

“Cordis” is a company; the AVANTI introducer is the catheter name. Like the PSI above, this catheter has an introducer and one side port.
Drop me a comment with questions! 🙂



I have had RNs and MDs argue with me about my ability to use a MAC for high pressure CTs. They tell me it is a Cordis so I can use it. Cordis is used interchangeably with an introducer so people think all Cordis are Ct pressure rated. That is not true. I think more education needs to be given. Cordis is a company that manufactures many types of lines (not just introducers), not all are pressure rated for CT. This was verified by our iv line specialist.
Does the side port on a venous sheath with a temporary transvenous pacer wire required a continuous KVO for patency? Our docs want them capped so the pacer wire won’t migrate. I’m struggling to find best practice for this particular instance.
I can’t imagine a KVO at like 5 mL/hr would cause a significant difference. Not sure if there’s even an evidence-based consensus on this, so I’d have to defer to individual hospital preferences.
Hi Rishi, I am working on QI on my unit (CVICU) trying to get invasive lines out of patients when possible. All our cardiac surgery patients come out with a RIJ MAC and Swan. Swan is usually pulled within a day and MAC as soon as no longer indicated. Sometimes we have patients that have prolonged pressor requirements so the introducer sheath stays for an extended period. It is my understanding that they are intended for short term use. Are there any guidelines for length of use or known complications of having a large bore catheter in the IJ for weeks at a time? Do you have a recommendation for alternative? Often times patients will get a PICC inserted but there is one patient we have right now where an upper-extremity PICC is contraindicated because he will probably require long-term dialysis access.
Typically we leave these short-term central lines in for a week at most, and if patients need longer-term central access, we’ll discuss midline/PICC. If the imminent need for a PICC is greater than the possible need for long-term HD, then I’ll discuss the pros/cons with my nephrology colleagues. Alternatively, for longer term central venous needs (e.g., TPN), I might ask my vascular surgery colleagues for a Pro-Line. Another short-term option I use is peripheral pressors through an 18 G IV for 24 hours.
Dear Rishi
I am a polymer engineering student. I would like to know about the materials that are used to produce the sheath, What kind of polymers is applied in this product?
Sincerely yours
Hi there! I’m honestly not sure. If I find out, I’ll update this comment!
what causes blood or fluid backing up (infusing from the side port )in the catheter sleeve (pt has transvenous cath inserted)
I’ve seen this happen often when there is a significant difference between the transvenous pacemaker diameter and the diameter of the introducer being used (for example 10Fr introducer with a 5Fr transvenous pacemaker). If the pacemaker does not fit snuggly within the introducer’s rubber, the possibility of leakage is greater. In my experience, 8.5 Fr Arrow’s percutaneous sheath introducers are an excellent choice to avoid this issue.
Can I place a transvenous pacer through the MAC? I’ve heard the MAC is larger French than the transvenous pacer so there is no true seal and air can get through or blood can back flow?
Pacing sheaths are smaller than the MAC (see some examples from Arrow). Introducers typically have a one-way valve that prevents backbleeding when something is passed through it (a Swan, introducer catheter, etc.), but I’d still use pacing wires with a sheath they are designed for.
There are Tuohy-Borst adapters to be able to use smaller pacing wires through larger introducers but they don’t work very well. You should follow the manufacturer recommendations to match introducer/sheath size to pacing wire size. I used to put bright orange signage with a stop sign at supply machines for the 2 introducer sizes we carried (8.5F- THIS SIZE FOR PA CATHETERS & MTP) (6F- THIS SIZE FOR PACING WIRES)
What are the differences between arterial and venous sheaths? When would a patient in the ICU have one of these left in?
They might be left in following procedures that needed arterial or venous access. For example, it’s customary for electrophysiologists to place multiple venous sheaths (for ablation, intracardiac ultrasound, etc.) whereas for a procedure like a transcatheter aortic valve replacement (TAVR), arterial and venous sheaths might be left in place. When I’m in the ICU, if a patient has an arterial sheath, I transduce it like an arterial line. If they have a venous sheath, I can use it like a central line (fluids, meds, etc.) These sheaths come in various sizes too, so removing them might also involve surgical repair.
Hi Rishi,
Great article, I’ve followed you on Instagram and am always learning from your page. I’m curious about your thoughts on bedside CVICU RNs placing SLICs. I cannot seem to find any articles relating to this, and am concerned that this falls outside their scope of practice. Thoughts?
Thanks for your support! I don’t know the policy, but personally if you ask me, it’s riskier taking out a Swan than putting in a single lumen introducer catheter (SLIC) since the catheter can only go in where the introducer has already been placed (e.g. subclavian vein). It’s a 60 second, low-risk procedure whereas placing the original introducer (sheath, MAC, etc.) has many more risks.
Hi: Unless the CVICU RN is also a certified nurse practitioner or CRNA, this likely falls outside of scope of practice. I am an APRN (CNS-BC) and the one class that my ACNP classmates had that I did not was the one where they learned to insert lines and read MRIs. A BSN would not have had anywhere near the training to insert a central line.
Hi Whitney, I think they were referring to SLIC (single-lumen infusion catheters). It may vary from facility to facility but at ours, our ICU RNs can insert a SLIC or a blue obturator once a Swan-Ganz catheter has been discontinued. I prefer a SLIC because it gives yet another IV line as opposed to capping it off completely with an obturator.
I’d argue pulling a Swan is riskier than placing a SLIC through an indwelling sheath. ICU nurses I’ve worked with do both. Also, ONE class to read MRIs/insert lines??
Hello,
I am unable to find ANY info on the PSI or Flow Ratings for the Cordis Avanti + Sheath Introducer. Do you have any documentation stating the PSI or Flow Ratings? We are wondering if we can use it for CT Contrast injection rates of 5 ml/sec which translates to 18,000 ml/hr. So in the above information on the MAC, we are only able to use the brown port. I need to know the rating of the Cordis and if it more like the brown port or the smaller ones from the MAC that we cannot use.
Thanks!
Hey Sarah! Though I use the PSI and MAC regularly in practice, the Cordis AVANTI is not a catheter I have ever used. Unfortunately, I don’t know the flow rate nor was I able to find anything through a quick search.
Good explanation, thank you.
I am wondering if the 3 lumen catheter use for PSI is the same one used for MAC, or if we can use indistinctly ?
I’m pretty sure the “companion catheter” (up to 3 additional lumens) can be used for either one. ARROW definitely makes one for the MAC which I’ve used countless times, but off the top of my head, I don’t know if it definitively fits the PSI.
Hi Rishi!
I was googling and I come across your face! Thanks for this info. Helped with my documentation. Hope all is well! -BWH RN
I’m glad it helped! I miss BWH and Boston so much! Please stay safe!
Can I place a regular multiple lumen CVC into the sheath?
You can, but there isn’t a way to “lock” the CVC into the introducer since they’re not designed for such a purpose. There are specially designed catheters (ie, SLICs) which interface with the locking mechanism on the introducer and should be used instead.