
Reexpansion pulmonary edema (RPE) is a rare but potentially life-threatening condition that occurs when the lung is rapidly expanded following compression due to air (pneumothorax) or fluid (pleural effusion). Although the underlying pathophysiology is poorly understood, it is attributed to increased alveolar-capillary membrane permeability, reperfusion injury, and even surfactant dysfunction. It has been shown that the incidence of RPE is independent of the volume of fluid removal – we need to focus on the rate of removal.
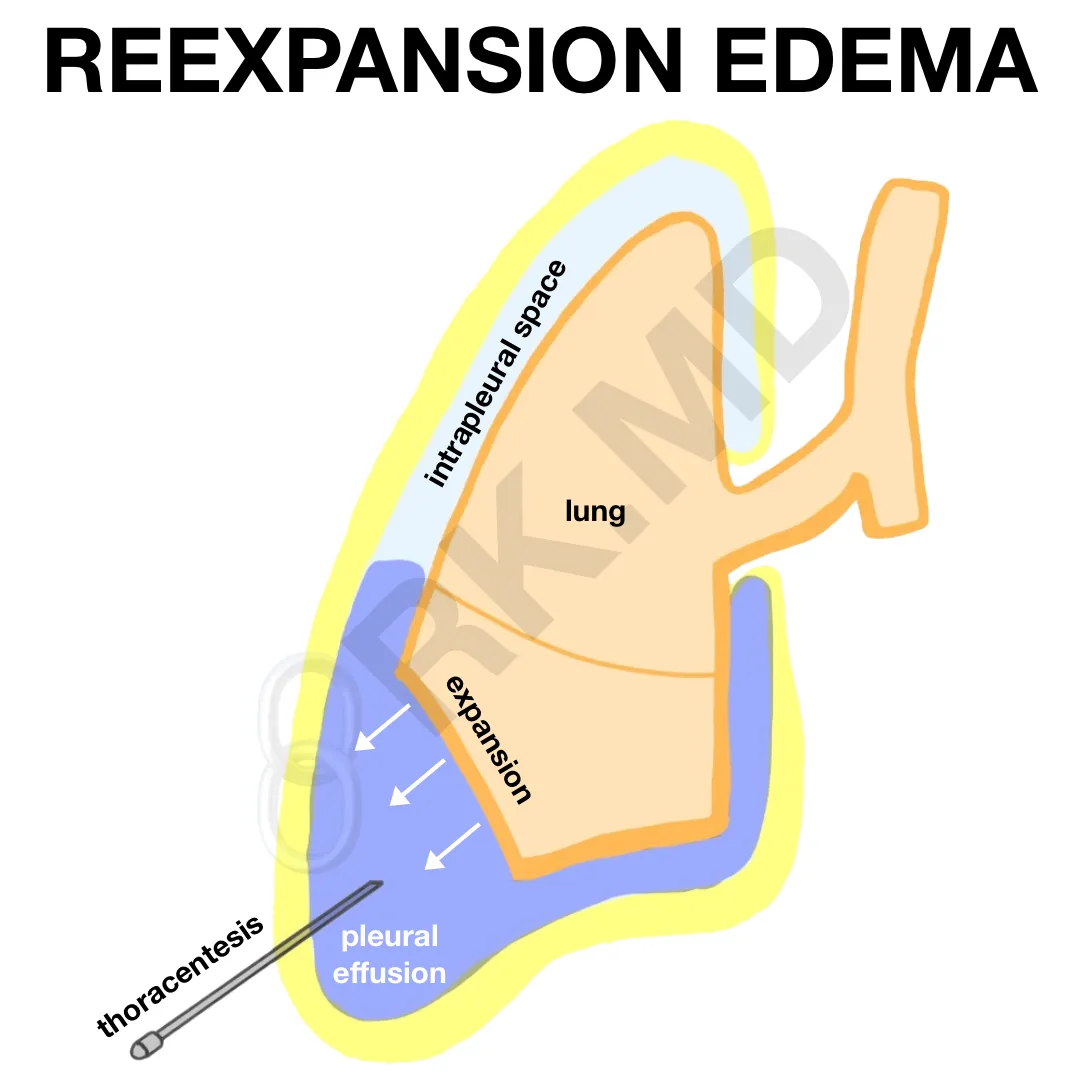
Symptoms of RPE include dyspnea, chest pain, pink frothy sputum, coughing, and diffuse alveolar infiltrates on chest radiograph. Management is centered around supportive care ranging from supplemental oxygen to positive pressure ventilation with diuretics. To minimize the risk of RPE, one should focus on a gradual, controlled expansion (especially in younger patients with prolonged lung collapse).
As an intensivist, as I’m draining and monitoring the resolution of pleural effusions with ultrasonography, I look for symptoms of reexpansion (e.g., cough) and temporarily pause drainage. After the patient equilibrates, I’ll gradually resume drainage as clinically indicated to avoid RPE.
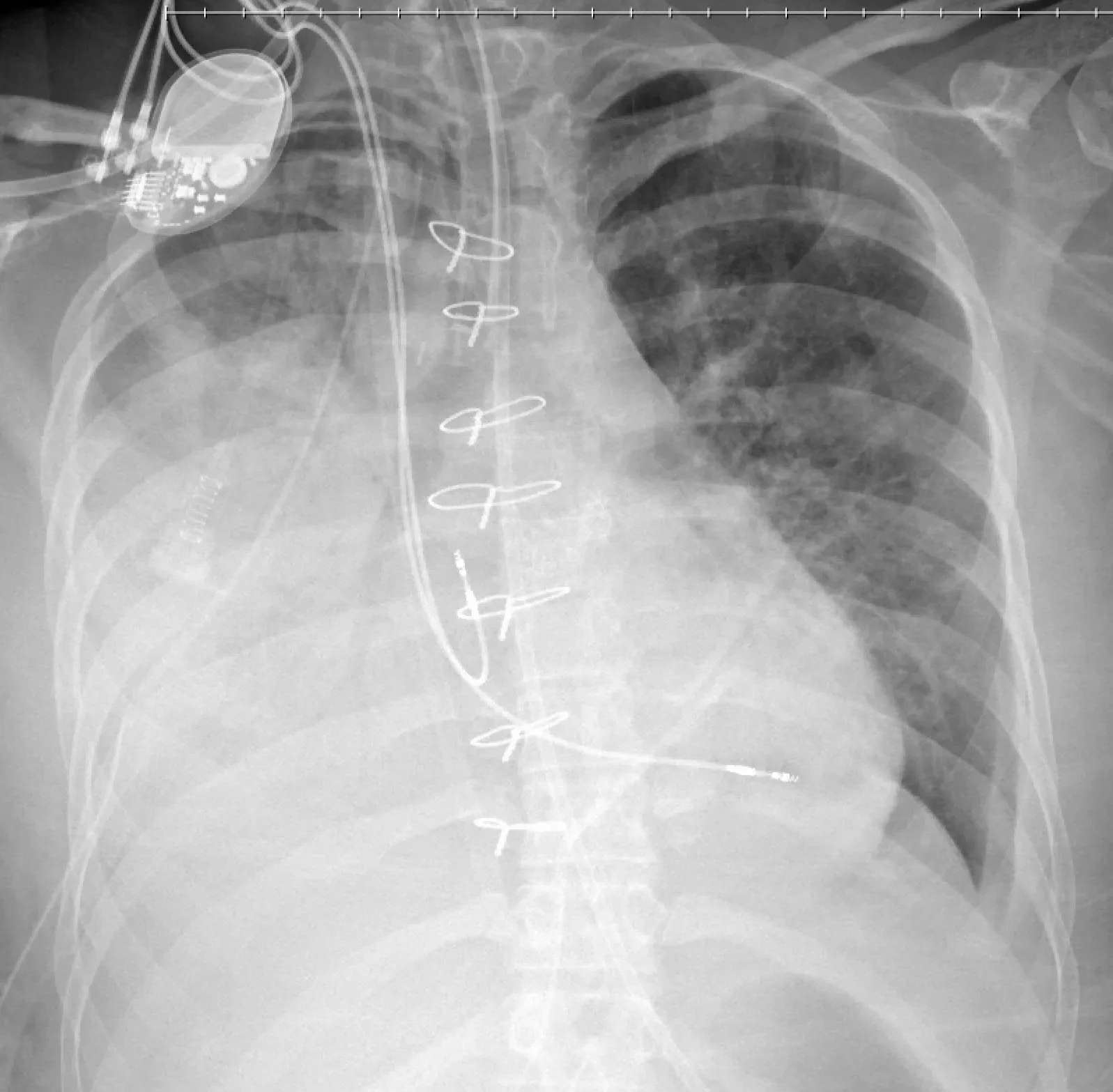
This is a chest x-ray in a case where 750 mL of right-sided pleural effusion was rapidly drained leading to profound hypoxemia and frothy sputum consistent with RPE.
Drop me a comment below with questions! 🙂



How I drain 500 ml every 30-60 min. Practically
I use a stopcock to stop draining. I’ll assess the patient every half hour or so and drain more if warranted.
Can you delivered us lecture on
Tisagenlecleucel gene therapy?
Sorry but I don’t have any experience with that particular therapy!
Any relationship between this and so called “robo lung”, i.e. pulmonary edema after re-expansion of nonventilated lung after a long period of one-lung ventilation?
I read if we do thoracocentesis more than 1000 cc at first time will result lung edem
That’s why I don’t do more than 1,000 cc initially. This conservative approach doesn’t prevent re-expansion edema, but just makes us feel better. 😉