
In any basic pharmacology course, we’re taught the concept of an “elimination half-life,” or the time it takes to reach 50% of a drug’s initial concentration. However, with more advanced multi-compartmental models of pharmacokinetics, the concept of a “context-sensitive half-time” more accurately describes the interplay between a drug’s distribution in the body’s compartments, metabolism, and excretion to reach the same 50% concentration endpoint.
A context-sensitive half-time describes the relationship that the duration of a drug infusion has on its apparent half-life. When we first start an infusion, the plasma and tissue concentrations are both zero. With the initiation of the medication (let’s say a propofol drip), the plasma concentration increases, and some of the propofol is rapidly metabolized by the liver. High plasma propofol levels will subsequently transfer to vessel-rich organs, fatty tissue, etc., based on concentration gradients.
When the propofol infusion is stopped, plasma concentrations will begin to fall. This will favor the transfer out of the peripheral tissues back into the plasma. Now, propofol will continue exerting its effect even though the intravenous infusion was stopped. Coupling this with ongoing metabolism, distribution, and excretion, one can see that many factors are at play. The context-sensitive half-time reflects the cumulative effects of these factors.
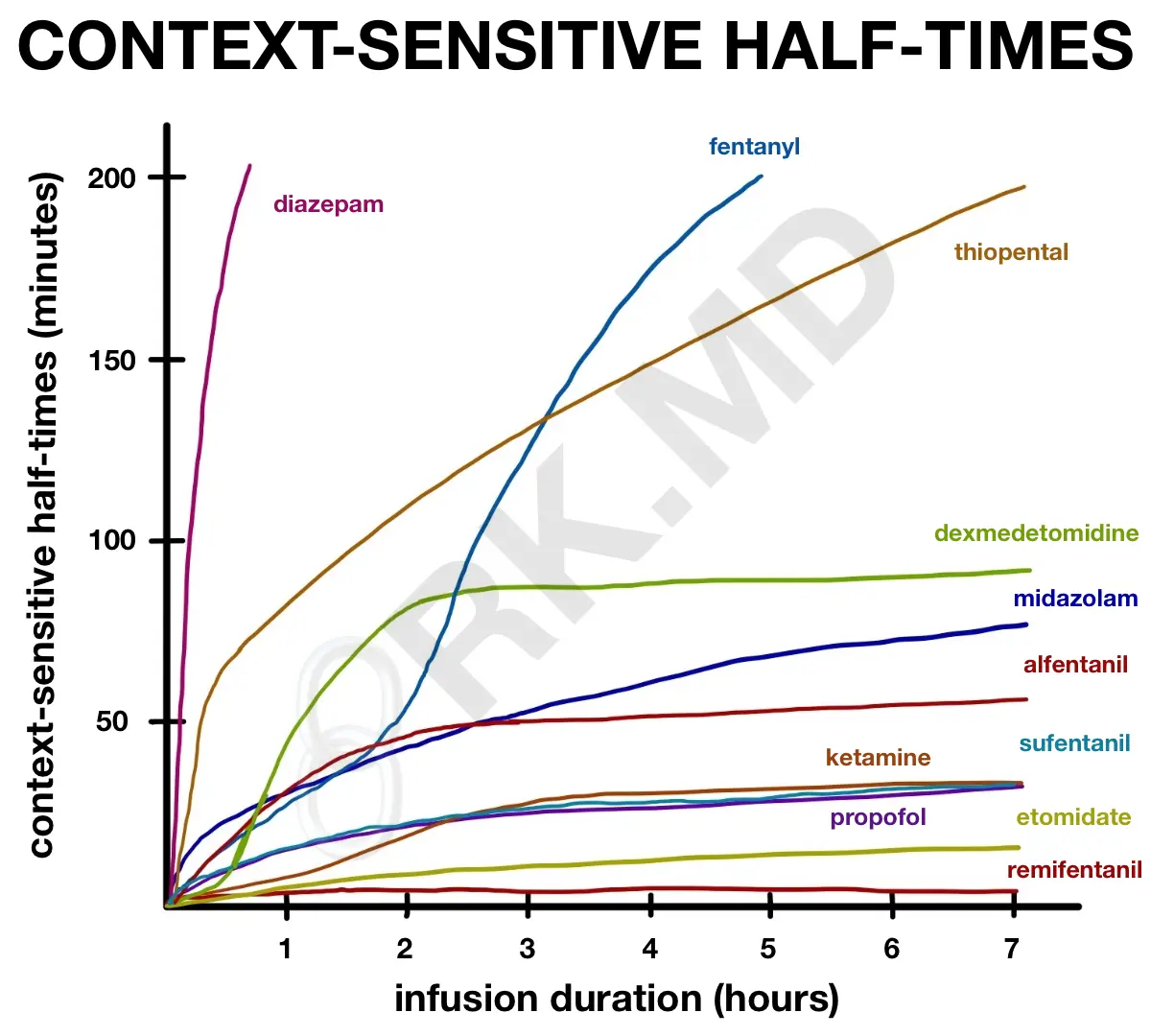
This concept is dramatic with lipophilic drugs like thiopental, diazepam, and fentanyl. In the case of fentanyl, after an infusion of 2-3 hours, its context-sensitive half-time skyrockets due to the depot of fentanyl in peripheral tissues. This is why I’m against using fentanyl drips for sedation in patients requiring mechanical ventilation. If the drip has been running for a while, it will take MANY hours before the patient is ready to extubate after discontinuing the sedation.
Drugs like remifentanil are unique because, as shown in the figure, its context-sensitive half-time is independent of infusion duration. In other words, it doesn’t matter if you run remifentanil for 2 hours or 10 hours; it has a context-sensitive half-time of 3-4 minutes. Remember, this tells you nothing about whether the plasma level you achieve is within the drug’s therapeutic window (i.e., is it actually providing analgesia in the case of remifentanil?)
Next time you run an infusion of ANYTHING, remember the concept of context-sensitive half-times! 🙂



Dr Kumar, I’m a great fan of your blog. I would like to know which drug you like to use for analgesia in mechanically ventilated patients in the ICU. In my practice we always use fentanyl but as you have showed, it has a great context-sensitive half-time after a few hours. Thank you
Hey Victor! Thanks for the great question! For hemodynamically stable-ish patients, I prefer a propofol drip with intermittent fentanyl boluses (as needed, NO drips) or dexmedetomidine drips. Although I avoid benzodiazepine drips because of delirium and fentanyl drips because of its context-sensitive half-life, sometimes we have to resort to this in highly unstable patients (ie, trauma, post-cardiac cases with high vasopressor requirements, etc.)