
Loop diuretics like furosemide (Lasix) and bumetanide (Bumex) block the reabsorption of sodium, potassium, and chloride in the thick ascending limb of the loop of Henle. This interferes with concentrating the renal medulla, and in turn, disrupts the osmotic gradient that typically moves water from within the tubules to the interstitium. More water left in the tubules = more diuresis.
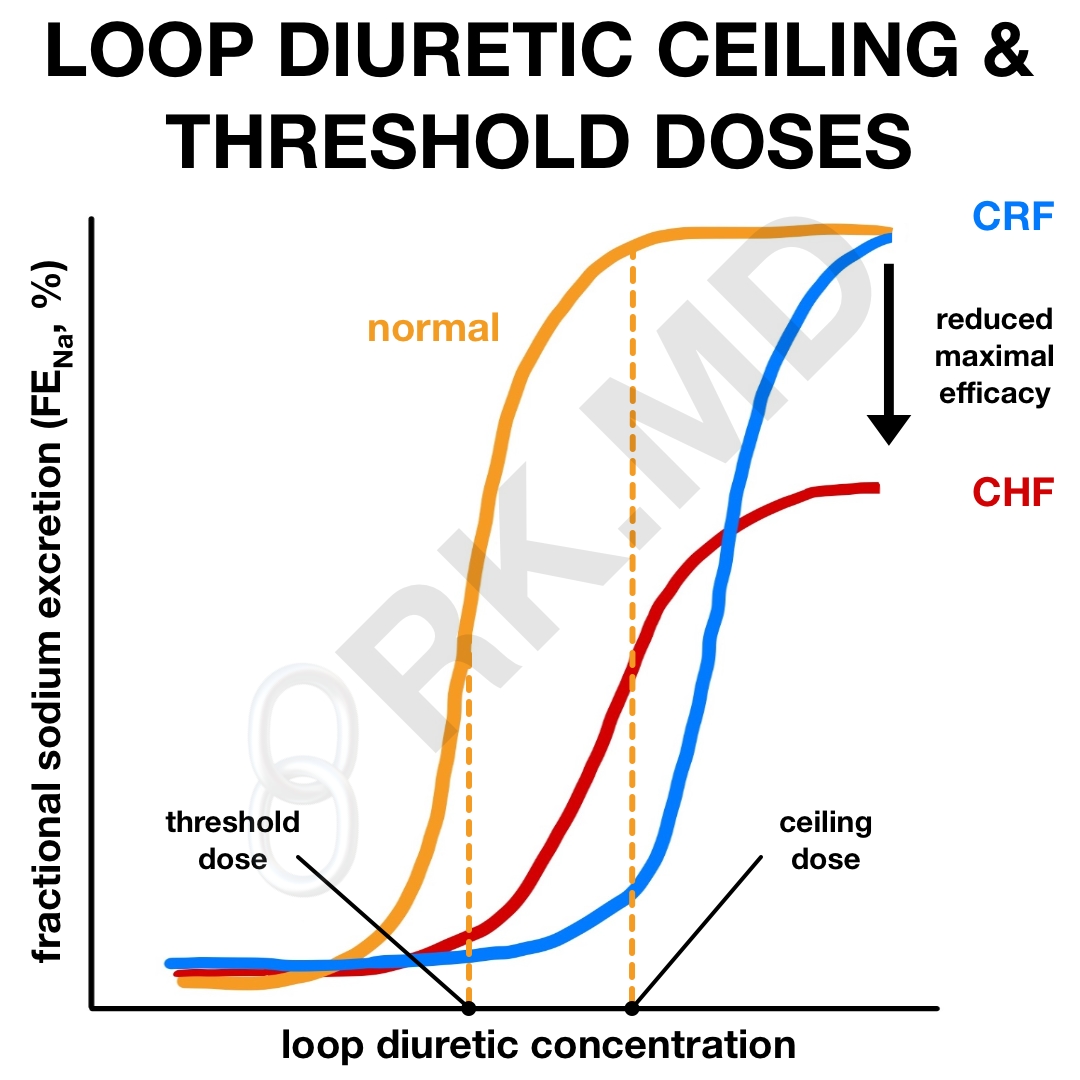
These medications follow a sigmoidal dose-response curve. At low doses, very little diuretic effect is achieved. Once a “threshold dose” is administered, diuresis begins to increase significantly. At some point, this effect plateaus and a higher dose won’t confer additional diuresis (and may increase undesired side effects!) This is termed the “ceiling dose.” In this chart, the fractional excretion of sodium (FENa) is used to gauge the extent of diuresis.
Keep in mind that threshold and ceiling doses can vary tremendously based on a patient’s comorbidities and current clinical status. In healthy patients, 10-20 mg IV Lasix should be sufficient. However, in chronic renal failure (CRF), I’ll use a higher dose (e.g., > 80 mg IV Lasix) to increase tubular secretion since the renal delivery of loop diuretics is reduced. In cirrhosis and congestive heart failure (CHF), the ceiling dose may be encountered at lower doses (< 80 mg IV Lasix).
In patients who are seemingly “resistant” to loop diuretics, I’ll either increase the dosing frequency or combine them with diuretics that work in other parts of the kidney (e.g., acetazolamide and metolazone) to create a sequential nephron blockade.
Drop me a comment with your thoughts regarding loop diuretics!


