
Thromboelastography (TEG) is a simple way of assessing many parts of the coagulation cascade from primary and secondary hemostasis to fibrinolysis. Thrombus formation typically requires four components: platelets which form the initial hemostatic plug, clotting factors that reinforce the platelets, fibrin which serves as a hemostatic glue, and other clot-supporting cells. I’ve used TEG to help in cases ranging from trauma and cardiac surgery to obstetric hemorrhage.
TEG examines each phase of the clotting process by introducing blood into a sample cup. The cup oscillates slowly (to simulate sluggish venous flow) around a submerged torsion pin. As coagulation occurs, the pin adheres to the clot and moves. The magnitude of pin motion is directly related to the clot’s strength. Amplitude decreases as fibrinolysis begins, and the pin starts to slip.
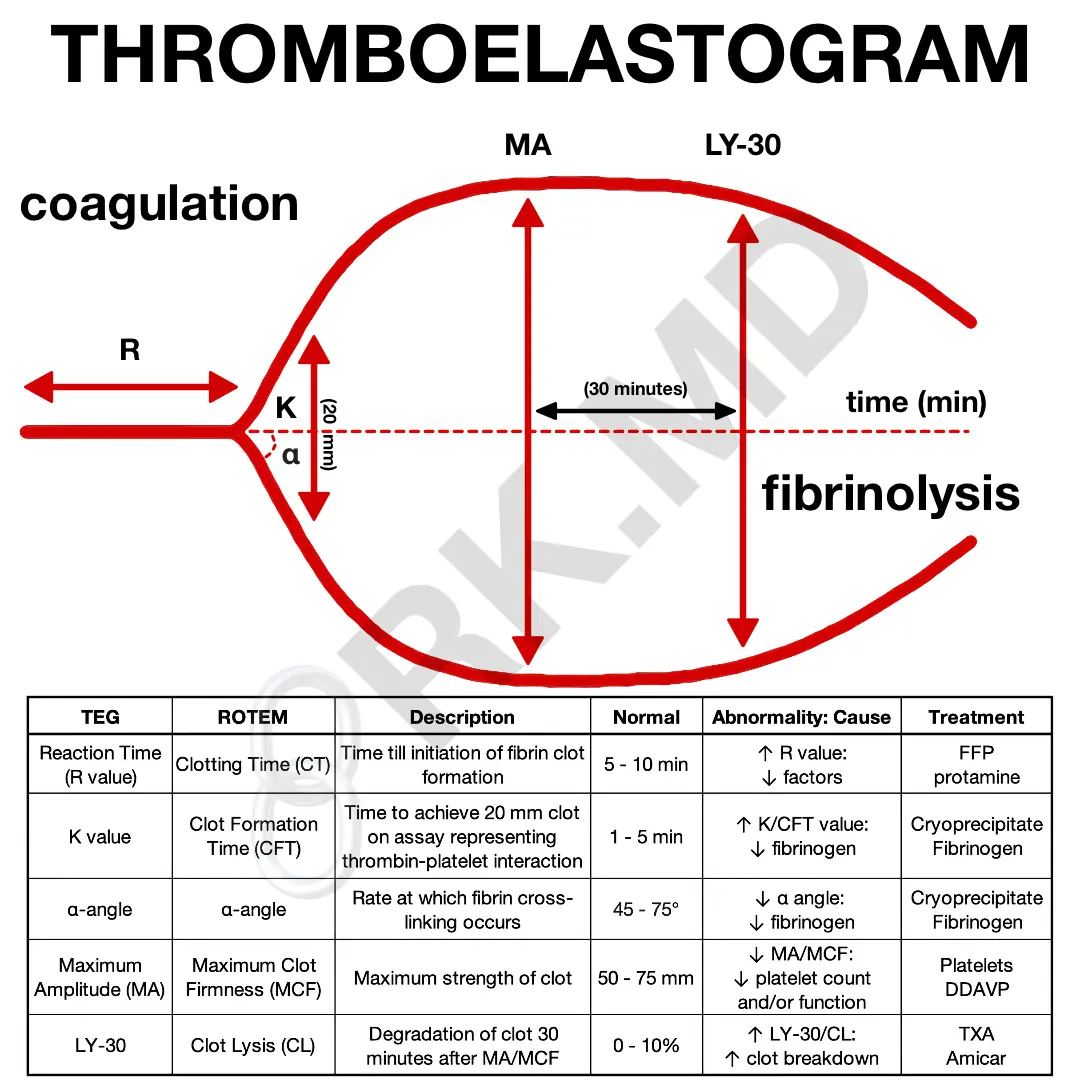
So, how do we interpret TEGs? Here are the five parameters:
- R (reaction time): time elapsed till clot initially forms. If the R time is elevated, this implies a deficiency in clotting factors. Replace them with fresh frozen plasma (FFP).
- K (K time): time elapsed till the clot reaches a fixed strength of 20 mm. If elevated, fibrinogen is low. Replace with FFP/cryoprecipitate.
- Angle (clot kinetics): speed of fibrin accumulation. A low angle implies low fibrinogen. Replace with cryoprecipitate.
- MA (maximum amplitude): highest vertical amplitude. Low MA implies a qualitative or quantitative defect in platelets. Replace with platelets and/or DDAVP. A platelet function assay (PFA) may also be helpful to run.
- LY30 (lysis 30 minutes after MA): percentage of amplitude reduction 30 minutes after MA. Measures fibrinolysis. If high, treat with antifibrinolytics like aminocaproic acid or tranexamic acid (TXA).

While TEG is a practical intraoperative test, it has some apparent limitations. Depending on the sampling technique, coagulation may begin before introducing the sample into the TEG machine. Furthermore, heparinized blood will require a heparinase before the assay. Since clotting is artificially activated (usually with kaolin) instead of von Willebrand factor (vWF), vWF disease will go unnoticed. Nevertheless, understanding TEG assays remains crucial to addressing coagulation anomalies.
As always, drop me a comment below with questions! 🙂



Thank you for your work. Can I ask you If I can use the figure in my research؟
Yes with appropriate credit! Thank you!
Ver helpful, do you. have cases to share so i can practise?
You’re the best Rishi! Your educational content is easy to digest, and has helped me throughout my perfusion program!
I really appreciate the kind feedback, and I’m so glad to know you find the content helpful! 🙂
yourr way of explanation is simply superb
Appreciate it! 🙂