
When exchanging an endotracheal tube (ETT) for a new single lumen tube (SLT) or double lumen tube (DLT), a paramount concern is losing the patient’s airway. Most institutions use some form of an exchange catheter to facilitate ETT exchanges, and in my training thus far, Cook catheters have been the way to go!
Practitioners often dismiss the real dangers associated with the ETT exchange process. Jamming a Cook catheter into an existing ETT, pulling out the old tube, and railroading over a new tube sounds easy enough, but there are a few key areas where things can go wrong, namely encountering resistance when passing the new ETT. Keep in mind that some of these patients have had tubes for extended periods of time, so their airways are friable and edematous at baseline.
My process for exchanging tubes is very methodical and straightforward:
- Make sure the patient is stable enough for ETT exchange from a cardiopulmonary standpoint.
- Preoxygenate the patient through their existing ETT.
- Make sure equipment is ready to perform a standard intubation (laryngoscopes, tubes, stylets, oral airways, LMAs, suction, etc.).
- Induce the patient with a hypnotic (propofol, etomidate, ketamine, etc.) and a paralytic (succinylcholine).
- Pass the Cook catheter into the ETT lumen. Gently advance the catheter until the depth has reached several centimeters passed where the existing ETT was taped at the mouth. This ensures the tip of the catheter is well within the trachea prior to further instrumentation.
- Obtain a view of the glottis with a laryngoscope. I often use a video laryngoscope for this purpose, but a standard Mac 3 or Miller 2 works well in most cases. You should see the ETT passing into the glottic aperture with the yellow Cook catheter within it.
- Deflate the existing ETT’s cuff and pull the tube. Have an assistant gently push the Cook catheter into the trachea while simultaneously pulling the ETT out over it. Maintain a view of the glottis at all times.
- Have your assistant thread the new SLT or DLT over the Cook and gently glide it into the mouth. Once it reaches the vocal cords, gently rotate the tube through the glottis and into the trachea. This is all done under direct visualization. Connect the ventilator and verify placement with continuous capnography, a CO2 detector, auscultation, etc.
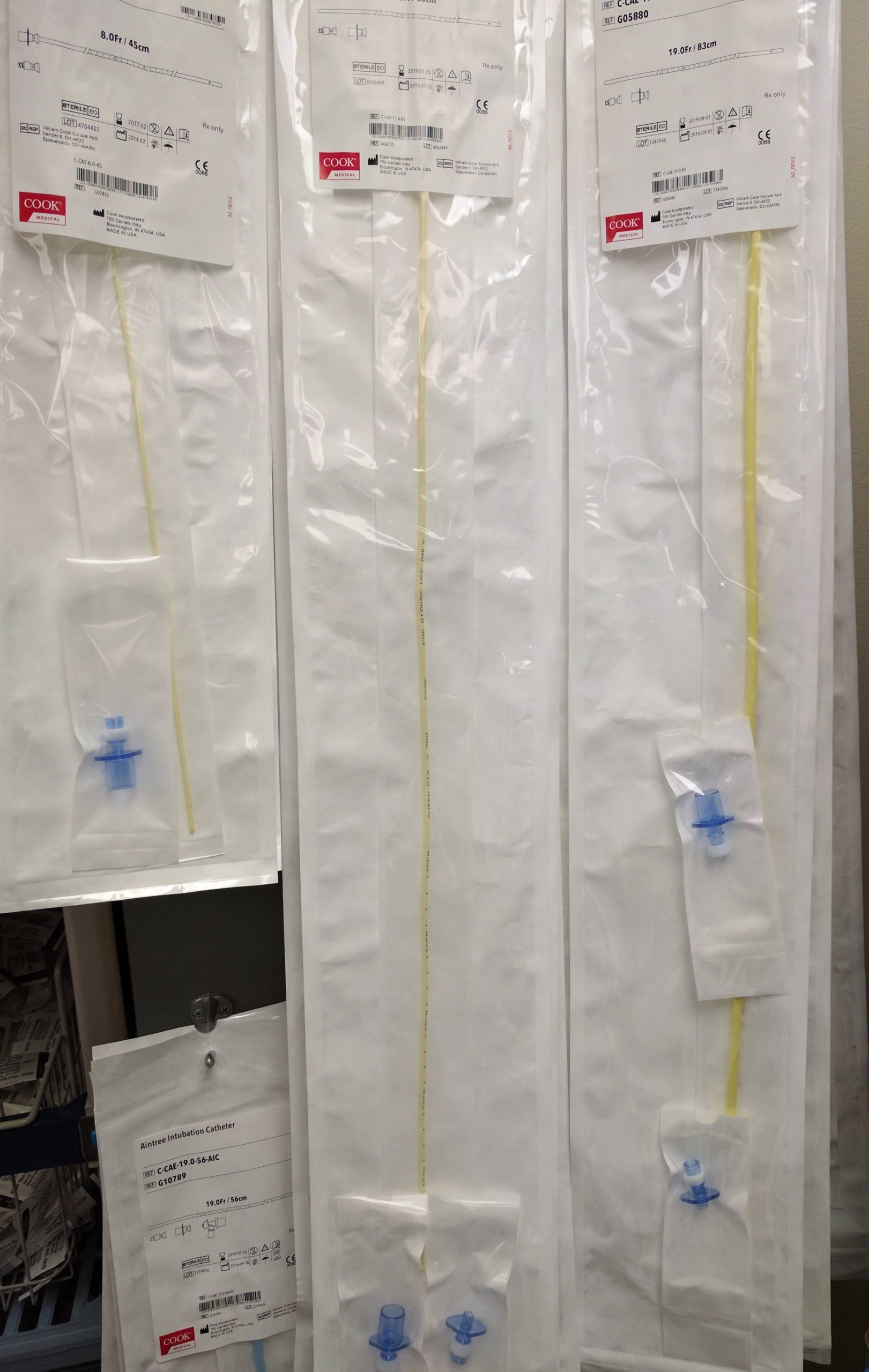
- If at any point your patient’s ventilation/oxygenation is compromised, you can ventilate through the Cook catheter using the blue adapter seen in the image.



Interesting…. In our structure we use for such procedure either a standard bougie or sometimes a nasogastric tube