
Synthetic human angiotensin II (Giapreza) is an intravenous vasopressor approved in late 2017 for septic or other distributive shock states. Normally, renin is released by the kidneys in response to decreased perfusion pressure in the renal arterioles, decreased salt concentration at the macula densa, and increased sympathetic stimulation. Renin cleaves angiotensinogen to angiotensin I, which, in turn, is further cleaved to angiotensin II by angiotensin-converting enzyme (ACE – yes, the same ACE which is inhibited by medications like captopril and lisinopril). Angiotensin II stimulates the release of aldosterone and is also a potent vaso/venoconstrictor.
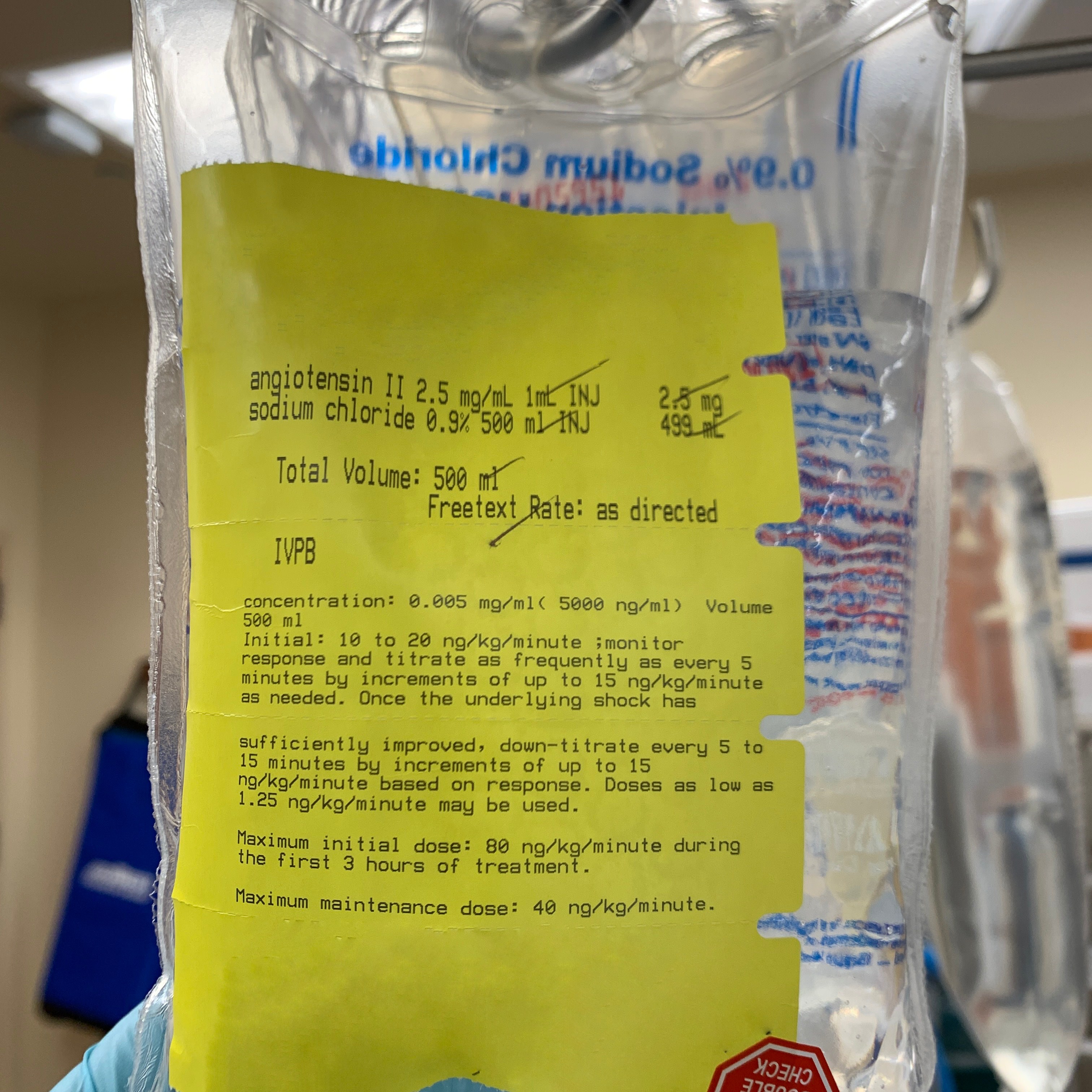
As a cardiothoracic anesthesiologist and intensivist, angiotensin II is a vasoactive agent I use in both the OR and ICU settings for patients with profound vasoplegia refractory to more conventional therapies like norepinephrine, vasopressin, etc. Dosing starts at 80 ng/kg/minute for the first three hours, followed by titration anywhere between 1.25 ng/kg/minute to 40 ng/kg/minute every 5-10 minutes. Given its extreme potency, I’ll only infuse this through a central line.
In the double-blinded ATHOS-3 RCT, patients with distributive shock who received angiotensin II versus placebo had a higher incidence of venous > arterial thromboses. Again, this stresses the importance of adequate VTE prophylaxis.
Once cost becomes less of an issue, I think this is the perfect drug to offset ACE inhibitor-related vasoplegia we often see under general anesthesia. Also, given its a hormone involved with several physiologic pathways, its clinical indications may be further expanded in the future.
Drop me a comment below with questions!



Would this be contraindicated in a patient with pulmonary hypertension?
Possibly! I can’t say I’ve used it enough to note a notable change in PA pressures. I’ll refer you to the FDA’s prescribing information regarding Giapreza (which doesn’t mention pulmonary hypertension).