Central venous pressure (CVP) or right atrial pressure (RAP) waveform tracings can oftentimes provide useful insight into a patient’s right ventricle (RV), tricuspid valve (TV), and overall cardiopulmonary status. The waveform morphology is easier to identify at slower heart rates and consists of three waves and two descents:
The waves generally represent filling or contraction, whereas the descents represent emptying or relaxation.
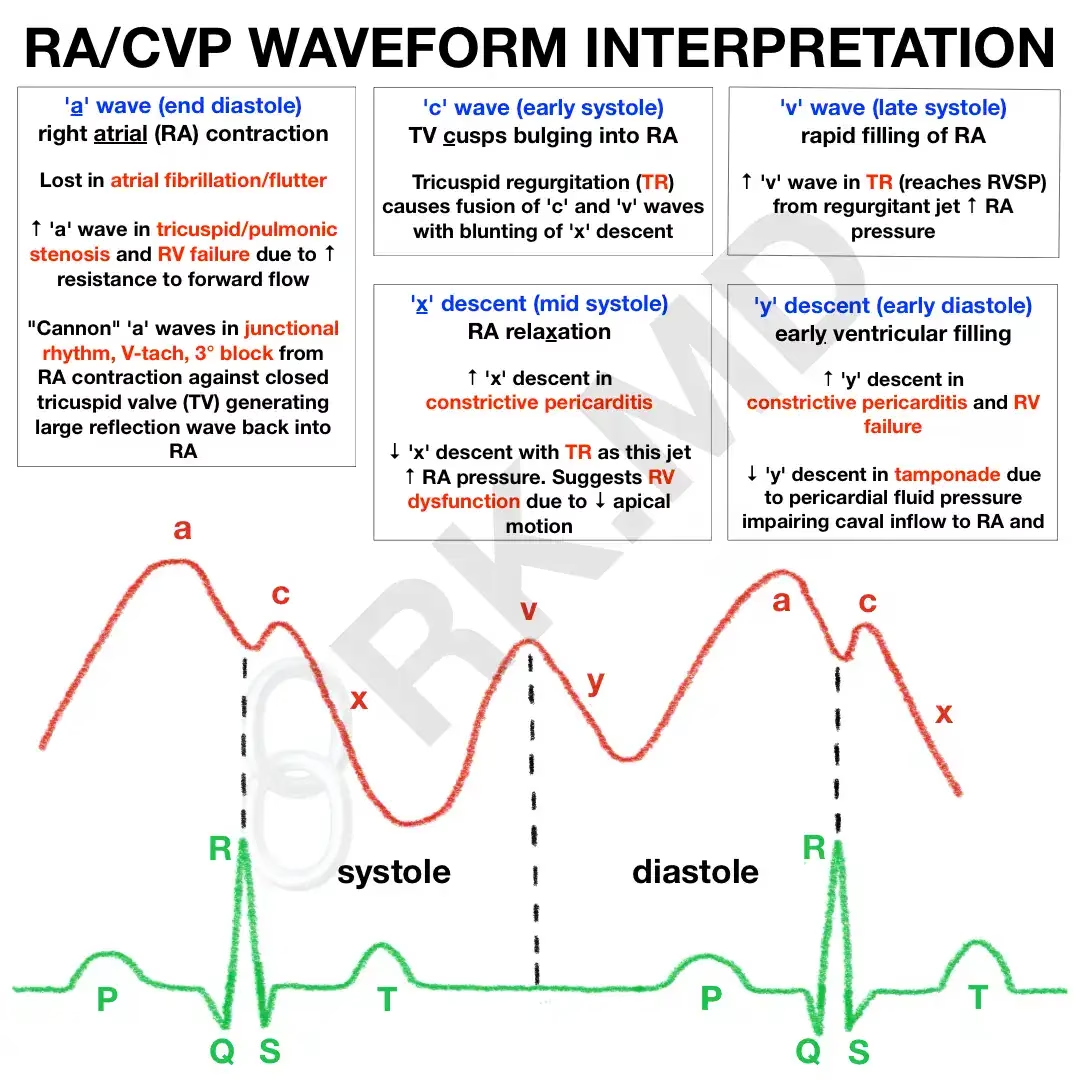
- ‘a’ wave (RA contraction at end-diastole): lost in atrial fibrillation/flutter due to disorganized atrial activity. ↑ in pathologies that impede forward flow like tricuspid/pulmonic stenosis and pHTN. Classic “cannon waves” caused by RA contraction against a closed TV causing reflection wave back into RA (junctional rhythm, V-tach, third-degree block)
- ‘c’ wave (TV cusps bulge into RA during early systole): c-v wave fusion and blunting of ‘x’ descent with TR
- ‘x’ descent (RA relaxation in mid systole): ↑ in constrictive pericarditis (CP), ↓ with TR (jet ↑ RAP) and RV dysfunction due to ↓ downward movement of RV
- ‘v’ wave (rapid filling of RA in late systole). ↑ in TR from regurgitant jet ↑ RAP. Similar tracings are obtained for LEFT atrial pressures (↑ ‘v’ wave with mitral regurgitation). The ‘v’ wave can gauge the success of mitral valve repair (e.g., MitraClip).
- ‘y’ descent (rapid RV filling in early diastole) Steep ↑ with constrictive pericarditis and ↓ with tamponade (↓ RV filling from ↓ caval inflow).
Drop me a comment with your thoughts and questions!

Leave a Reply