
Compared to internal jugular and femoral central venous catheters (CVCs), I prefer placing subclavian CVCs because they don’t tether patients’ necks, they’re easy to access, they’re easy to dress, and they’re in a part of the body that doesn’t “bend.” Subclavian vein cannulation is similar to epidural catheter placement in that they’re both difficult-to-teach procedures based on feel.
I’ll often scrub in with my residents/fellows to locate a good entry point, feel the clavicle with the finder needle, push down on the needle shaft to guide the needle below the clavicle, and above all else, keep their trajectory FLAT as they advance toward the sternal notch. Why? Because the apex of the ipsilateral lung is incredibly close to the needle’s path, and pneumothorax (PTX) is a very real risk. As with anything, don’t do a procedure if you can’t deal with potential complications. I’m comfortable placing a chest tube if need be.
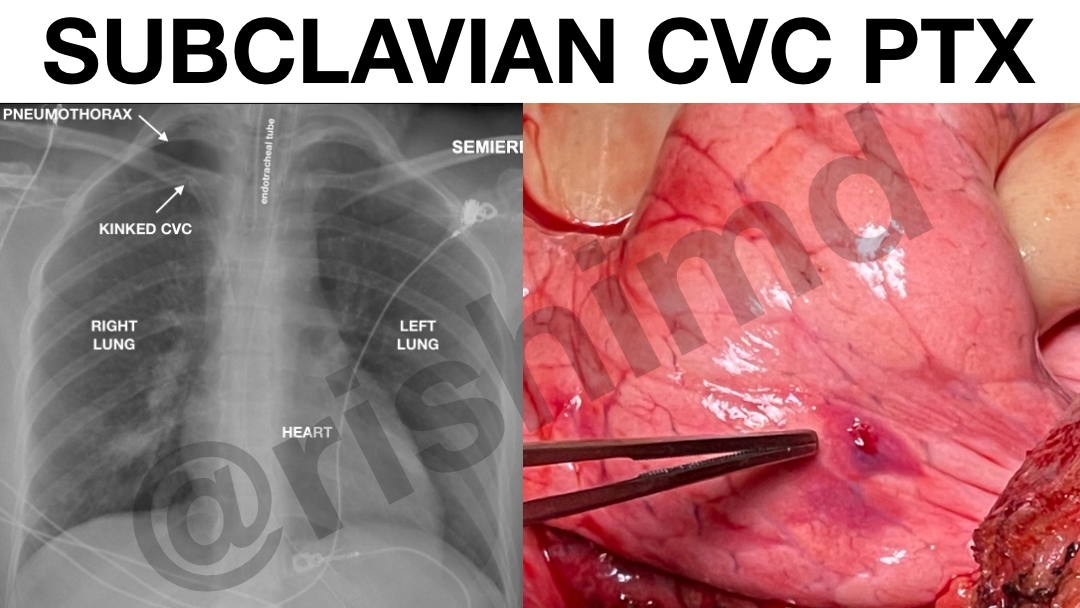
Here’s an example of a small, right-sided apical pneumothorax on chest x-ray (first image). The lung injury can be noted in the operative field as well (second image). This was due to a right subclavian CVC placement done by an outside proceduralist. Yes, ultrasound-guided (lateral) CVCs are a thing, but when I’m receiving patients from outside of the unit, I also have to address potential complications as they evolve under my care.
Drop me a comment below with questions!



Two questions:
In the ICU, is you first choice jugular or subclavian and second do hou us-guided or landmark technique for subclavian?
If it’s a patient I anticipate proning, then internal jugular with ultrasound. Otherwise, subclavian with ultrasound (unless it’s an emergency, then landmark checking with manometry).