
Normally, the intrapleural pressure (Pip), or the pressure in the space between the lung’s visceral and parietal pleural layers, is slightly negative relative to the atmosphere (Patm). This is due to the chest wall and lungs recoiling away from each other. During a forced expiration, expiratory muscles can increase the Pip (as noted in the diagram). This pressure is transmitted to the alveolus, increasing pressure within the airway. I’ve termed this bronchial pressure (Pbr). Flow occurs from regions of high pressure to those of lower pressure, so since Pbr > Patm, air is expired.
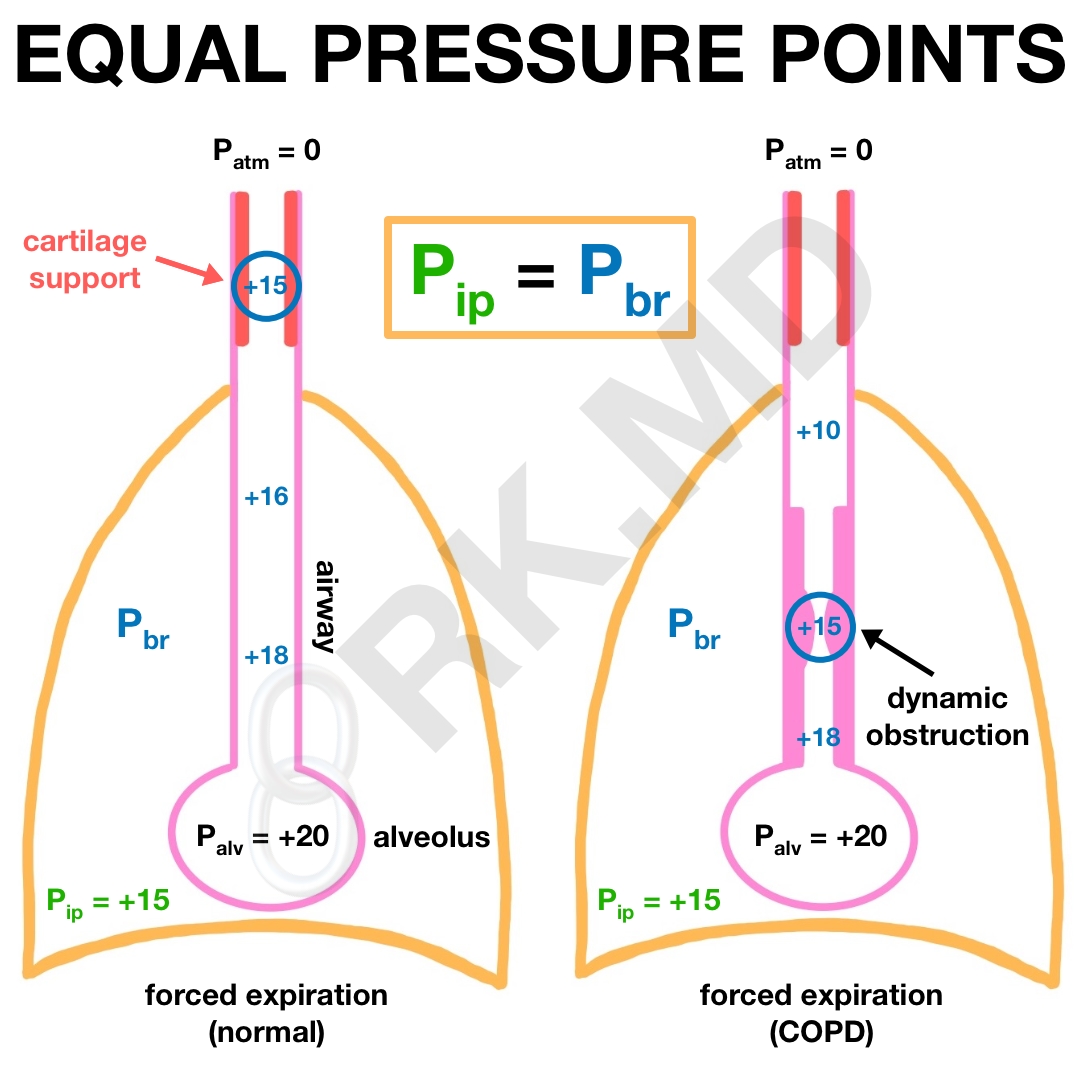
As air exits the lung (alveoli → bronchioles → bronchi → trachea), it encounters airway resistance causing Pbr to decrease. If the patient has obstructive physiology as in chronic obstructive pulmonary disease (COPD), expired air encounters more resistance leading to a precipitous drop in pressure (+20 down to +10 cm H2O, in this example).
In either case, Pbr stents open the airway, and Pip tries to collapse it. The point along the airway where Pbr = Pip is called the equal pressure point (EPP). Normally during forced expiration, the EPP occurs proximal in the tracheobronchial tree where cartilage reinforces the airway and prevents collapse; however, in patients with COPD, the EPP is much more distal, causing airway collapse near the alveolus (parts of the airway NOT reinforced with cartilage) leading to hypoventilation, hypoxemia, air trapping, etc.
This explains why patients with COPD habitually exhale through tightly pursed lips. By limiting the rate at which air is exhaled, the patient can maintain a higher airway pressure (Pbr) to help stent the airway where it wants to collapse.
Be sure to check out my other post on the basic physiology of breathing, and drop me a comment below with questions! 🙂



What happens to EPP is positive pressure ventilation?
Hi! Thank you for this explanation! It’s fantastic!! I have a question. Why is there a sharp drop of pressure in exhalation and why does this correlate with more resistance in the airway? Thank you!
This drop in pressure is termed “friction loss.” Read more in this free article.
I’ve watched multiple videos and I couldn’t get it for the life of me, but now it all clicks. THANK YOU SO MUCH! 🙂
I’m so glad you found it helpful! 🙂
This is the best explanation of EPP I’ve read! Thank you!
Thank you so much, Frank!
I’ve read about it a lot and this was the first time I understood the concept of equal pressure points. Thanks!
So glad you found this post helpful! 🙂
Rishi me too. Thanks for this. I am a RT student. Do you think your notes will be helpful through my program? I would like to access it, its put together better than class haha
Hey Dr. Rishi,
So I believe I understand this correctly, but let me know if I am wrong. I have the basic concepts down the difficulty comes when you talk about the Pbr working against the Pip to keep the distal airways open upon forced expiration. Is the Pbr pressure keeping the airway open because as PiP increases the air is forced from the alveolus and that is the air forcing itself forward as well as against the walls of the distal airways?
Then for the COPD patient you bring up, does the pursed lip breathing increase that Pbr by providing resistance to the outflow of air and increase the pressure in the system that way?
Thank you for your articles! Always a very interesting read and very easy to grasp!
Matt
Great questions, Matthew! I’ll start with your second one – yes, exactly. Pursing one’s lips maintains more air pressure within the airways (higher Pbr) to counteract the intrapleural pressure (Pip) that wants to collapse the airway.
Now to address your first point, Pbr is higher than Pip during forced expiration at the alveolar level, but the farther air traverses the airway (ie, moving from the alveolus to the mouth), the more pressure drop off occurs. At some point, the Pbr (pressure within the airway) is less than that outside the airway (Pip) leading to airway collapse.
Hi Dr Rishi!
Just wondering why the obstruction in the small airways causes the pressure to drop off more quickly in a COPD patient?
Cheers!
Patients with COPD have difficult breathing air OUT of their lungs, so I like to think that the airway pressure is higher in their distal airways (alveoli, respiratory bronchioles, etc.) compared to their more proximal airways (trachea, mainstem bronchi). With the dynamic obstruction, there’s some degree of airflow acceleration between the distal airways and proximal airways causing a larger pressure drop off (Bernoulli’s principle) to occur in the area with higher velocities (proximal airways). At least this is how I think about it… let me know if you find a better explanation! 🙂