
Ibutilide is easily one of my favorite drugs in critical care and perioperative medicine. It’s a short-acting “pure” class III antiarrhythmic (potassium channel blocker). Amiodarone is traditionally classified as a class III, but it possesses properties of other antiarrhythmic classes as well as a much longer half-life. Ibutilide can cause fatal dysrhythmias like torsades de pointes, so I usually coadminister several grams of magnesium with the drug.

One can imagine that in patients with chronic atrial fibrillation (AFib), even if we’re lucky to pharmacologically convert them back to sinus rhythm, there’s a high likelihood that they will revert to AFib. We must therefore weigh the risks and benefits of using ibutilide to convert these patients compared to alternative means of management (ie, rate control with beta blockers).
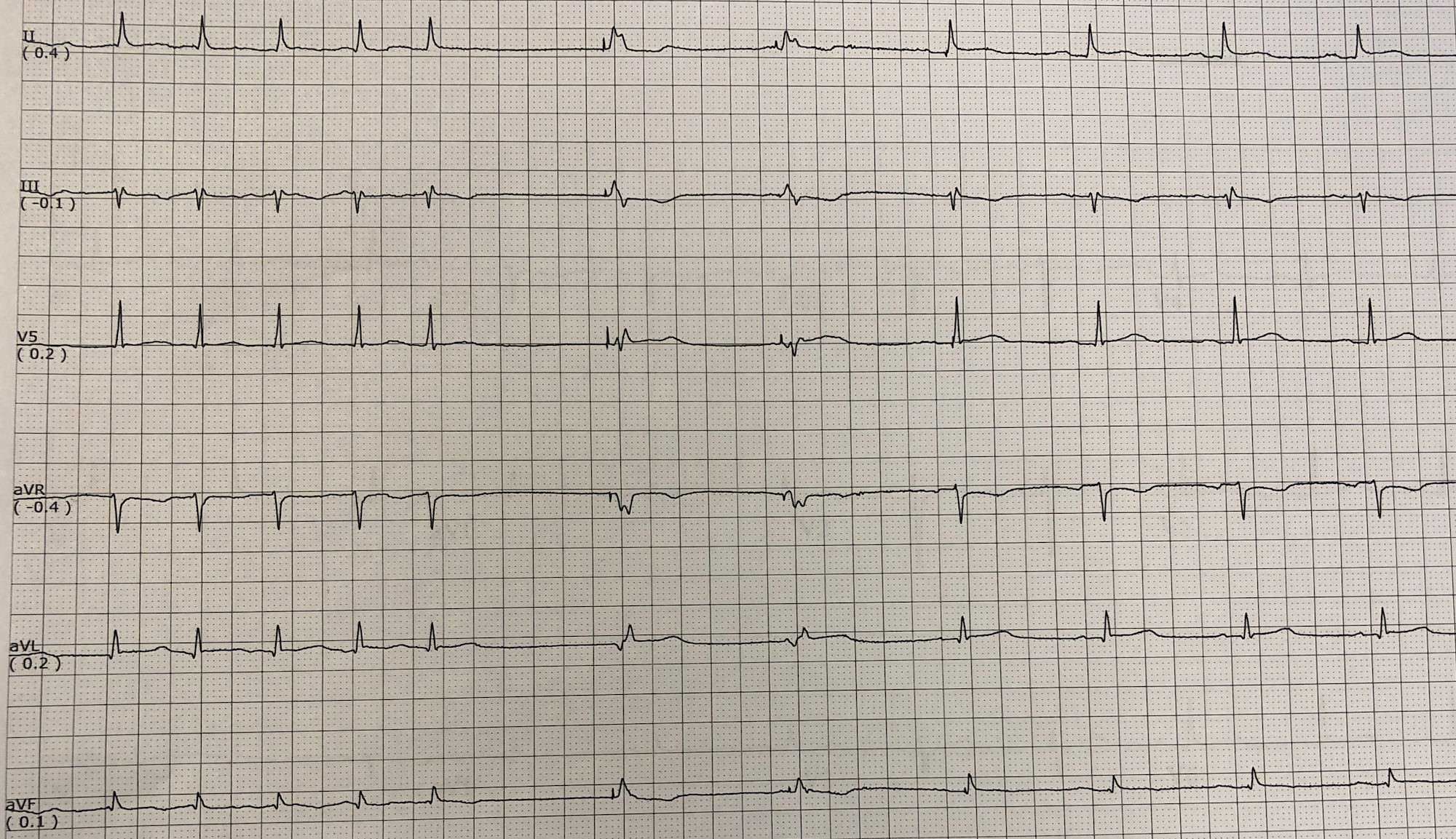
When I choose to go through with converting, I’ll give 1 mg of ibutilide as a slow push over several minutes, wait 30 minutes, and give another 1 mg if necessary. This EKG shows a case where I used two doses of ibutilide to successfully convert atrial fibrillation to sinus rhythm because I was struggling with perfusion pressures. 🙂



How much are several grams of magnesium?
2-4 grams of IV magnesium sulfate.
Dr.rish amiodarone very active and multiple action but approximately so many adverse effect.sotalol is unique drugs. why ibutilide ?u mention that it is most selective potasium ,but it’s all the same drugs. So ibutilide is the best medicine or just ur favorite drugs to use but all of this are contain same drugs?
Thank you and may god bless you to ur everyday saving life…
There are lots of options, but I personally like ibutilide for logistical reasons and its relatively short half-life. 🙂