
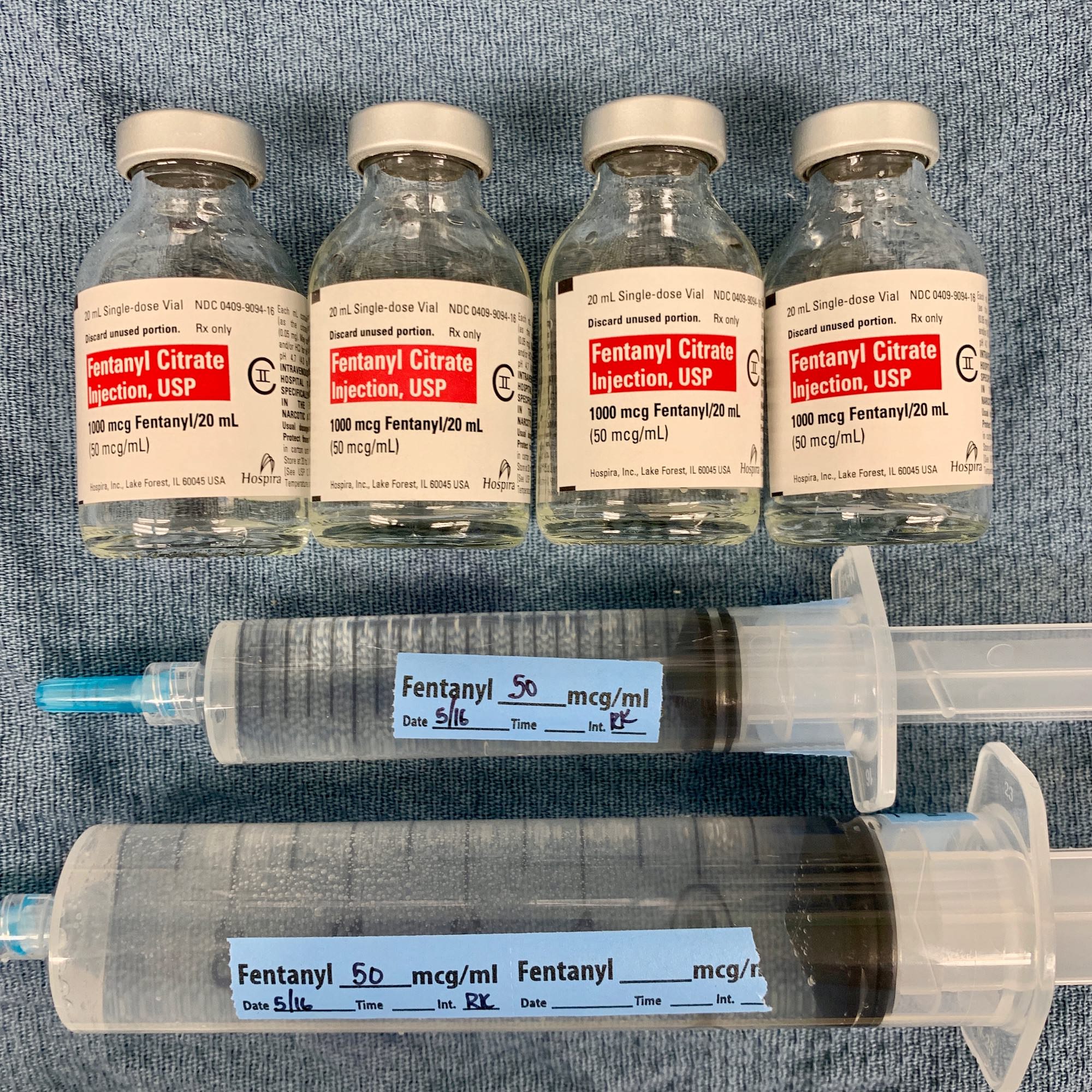
The induction of general anesthesia in patients undergoing cardiac surgery is often times different than non-cardiac surgery. At many institutions, these inductions tend to center heavily around high dose opioids due to the hemodynamic stability conferred by narcotics. When talking about fentanyl, this translates to anywhere from 50 – 100 mcg/kg. Yes, that can be upwards of 4,000 MICROGRAMS OF FENTANYL (as pictured!) Although fentanyl is typically regarded as a “short acting” agent, in these doses, significant uptake by fatty tissues with subsequent redistribution makes this a much longer acting narcotic.
In the era of enhanced recovery protocols and balanced anesthetics, this isn’t my preferred induction style; however, I’ve done it several times and am always impressed by the process. The most important consideration is the onset of chest wall rigidity – likely a central nervous system mediated spasm of the chest wall – which significantly limits our ability to ventilate. For these inductions, I usually give enough narcotic till the patient is unconscious, then push a neuromuscular blocking agent, and then complete the induction by securing the airway and minimizing the amount of volatile anesthetic I use.
Drop me a comment below with questions! 🙂



I would like use propofol with careful titration and pressor support.
That’s what I do the overwhelming majority of the time these days.
Hey Rishi! When pushing these large doses of fentanyl for induction, is it all one big continuous bolus, or do you have to go slow and pause after every few hundred mcgs and see how their hemodynamics respond? We often hear about how opioids are relatively hemodynamically stable, but I just wonder whether the key word here is “relatively”. Some insight about how this type of induction actually plays out in the OR would be awesome!
Great question! I only did the “high dose fentanyl” induction a couple times as a fellow, and usually did as you mentioned – 500 mcg and then check… 500 mcg more and then check. I don’t care what people say about it being hemodynamically stable – with enough opioid, you WILL see hemodynamic instability, chest wall rigidity, etc. These days, I might start off with 100 – 250 mcg with ~50 mg of propofol, rocuronium, lidocaine, and support (norepi, epi, calcium, etc.) After securing the airway, I’ll start some low-flow volatile (ie, 1% isoflurane at 1 L FGF) while placing additional lines/monitors.
Hi Rishi, very good information in this post, thank you for that. in my experience the high doses fentanyl inductions also provide excellent results on decreases the postoperative pain, of course, we need to keep in mind the pharmacokinetics of this opioid and the relation between it’s half-life and the surgical time. a inductions doses like you describe in the post reports benefits for my patients only when the surgery doesn’t prolong for more of 3 hours.
Thanks so much for sharing your insight! 🙂
Hey Dr. Rishi,
Do you use cryoanalgesia in your setting at all? I have only seen it used once in pediatrics. If so what are some cases you have used it on I am curious about contraindications. Thank you for all the free education much appreciated your my favorite ig account!
Hey Chasity! I’ve only heard/read about this technique but never seen it in real life! Thank you for the kind words! 🙂
I found it very interesting that cardiac patients remain stable during induction and throughout heart surgery when they’re given Fentanyl. I don’t remember this being the case with all narcotics that we used in the heart rooms back in the olden days. I think it’s a great med that gets a bad rap bc of folks thinking they can abuse it without consequences. Great post Rishi??????
I get questions all the time from patients regarding medications they will receive in the OR because of what they see on the news. I clearly don’t endorse recreational use of any of these powerful medications, but they’re indispensable in the perioperative and intensive care settings.
As far as the stability during induction, there can be some degree of instability depending on how attenuated the sympathetic nervous system becomes (hard to gauge ahead of time).