
Pulmonary embolism (PE) refers to an obstruction of the pulmonary arterial system and is the third leading cause of cardiovascular death. Patients can present with nonspecific findings; however, resulting pulmonary infarction, impaired gas exchange, and right ventricular failure can lead to rapid decompensation.

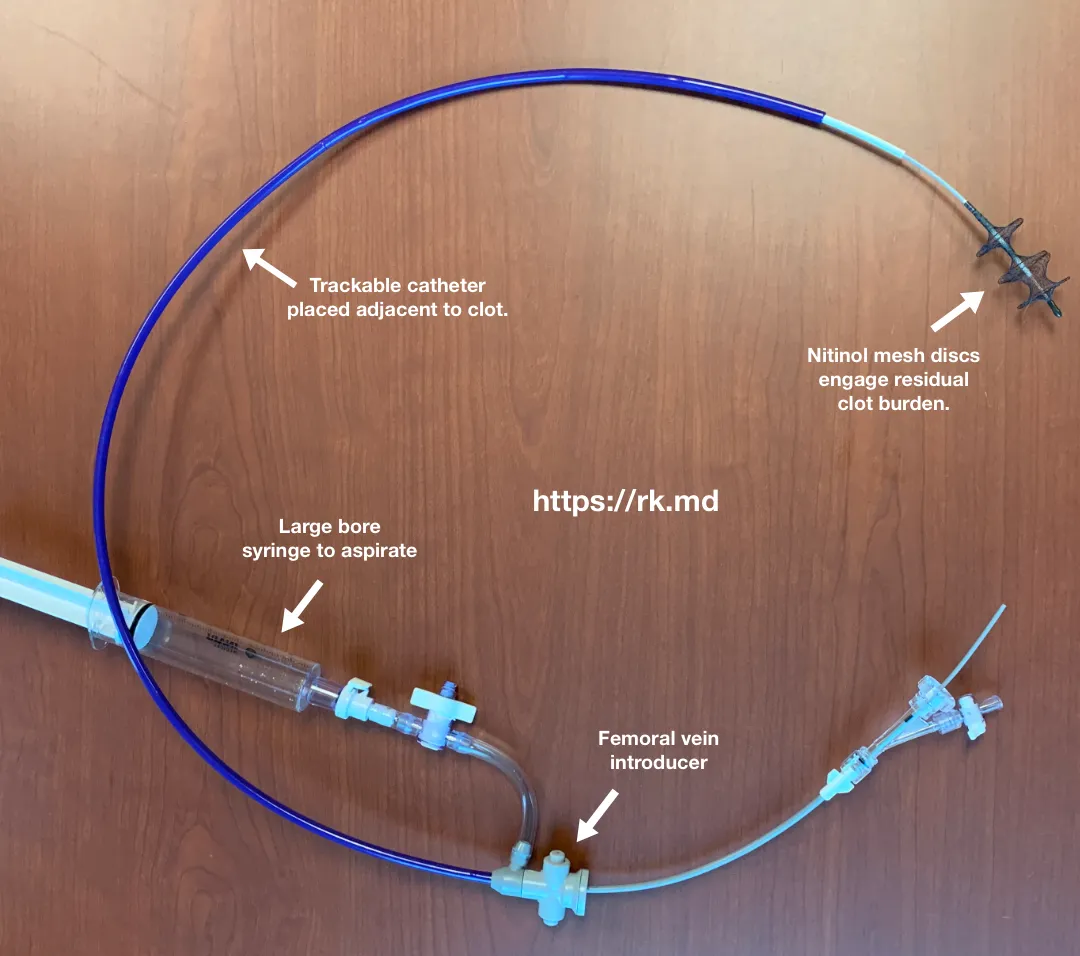
The Inari FlowTriever system allows proceduralists to perform a percutaneous, mechanical thrombectomy of this clot burden without thrombolytics. First, femoral vein access is obtained and a guide wire is advanced into the pulmonary vasculature with fluoroscopy through the clot. Then, a dilator is advanced over this wire to abut the clot. Suction is applied via a large bore syringe to extract the clot through the catheter. Finally, residual clot is captured with a second catheter containing self-expanding nitinol discs which “engage” the clot. These discs are pulled back into the trackable catheter dragging clot with them.
As a cardiac anesthesiologist, I perform monitored anesthesia care (MAC) for these patients with minimal sedation and lots of verbal reassurance. General anesthesia confers a very high likelihood of decompensation (positive pressure ventilation, decreased preload/inotropy, etc.), so I really want to avoid it. I’ll place a central line as many of these patients require vasopressors/inotropes, and an arterial line due to hemodynamic lability. Having blood available and a surgeon on standby is also paramount.
The 2018 multicenter FLARE trial looked at 106 patients with acute PE and echocardiographic evidence of RV strain (RV/LV ratio ≥ 0.9) who underwent the FlowTriever intervention. At 48 hours, there was a statistically significant reduction in the RV/LV ratio with no cases of intracranial hemorrhage, femoral vein bleeding, or device-related deaths.
Have you seen this system used before? Drop me a comment with your experience and thoughts!



Thanks for the article. I am an Interventional radiologist and getting anesthesia at one of our hospital can be difficult sometimes. Can you tell me what is your preferred vasopressor and antiarrthymics drugs and starting rates to use during procedures like this?.
Thank you in advance.
ER
There’s not a universal recipe for these cases (or any anesthetic). Some patients present in obstructive shock requiring judicious fluid administration with inotropic support (e.g., epinephrine 0.01 – 0.10 mcg/kg/min, although I’m reluctant to ever give doses because there are other considerations). I usually don’t reflexively use antiarrhythmics for these cases.