
During my ICU fellowship, in addition to reviewing all the orders during rounds, I also questioned the frequency of labs. Just because a patient is admitted to the hospital (especially an ICU) does NOT mean they need daily blood counts, metabolic profiles, coagulation assays, etc. In my opinion, this is a poor, cookie-cutter practice of medicine is an incredible waste of resources, time, and not to mention, causes iatrogenic morbidity for our patients (discomfort due to needle sticks, anemia, etc.)
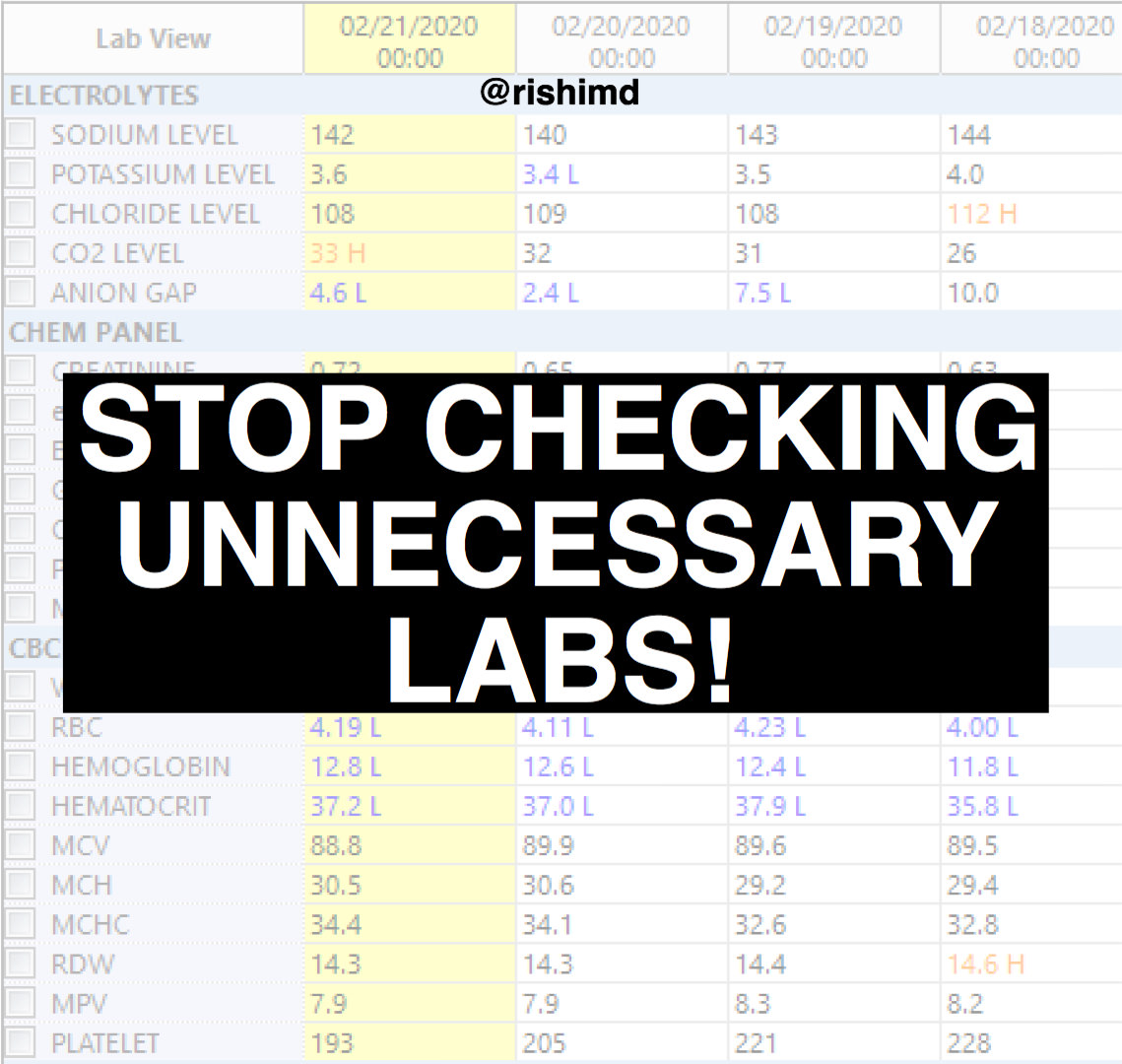
To drill this point home with my residents, sometimes I’ll open a chart, pull up the last week of normal labs, and ask them what abnormalities they see. After carefully looking for signs of infection, anemia, renal impairment, coagulopathy, etc., they’ll invariably answer: “Rishi, I don’t know. Everything looks okay.” And they’re exactly right. Why do we need to check daily labs in patients who are otherwise asymptomatic… or in every post-operative patient… or in situations where we’re not following an acute change?
We don’t need to!
I implore all healthcare workers to individualize care for the patient in front of you, be mindful of every order (fluids, medication, therapies, labs), and eliminate the knee-jerk impulse to order daily labs “just in case.”
Drop me a comment with your thoughts!



Thanks for writing on this; there are so many inappropriate labs ordered for inpatients, as well as perioperatively for outpatients! All of us should think instead of reflexively ordering labs. Thanks for your work.
Completely agree, Jordan! Thanks for the comment! 🙂
I’m a M3 so I’m pretty inexperienced but I think almost every patient I have had so far this year has gotten daily labs. I guess it’s just my institution’s culture. It does seem wasteful sometimes but I’d also be afraid of missing an early sign of something serious (GI bleed, infection, new drug causing rare side effect, etc) and sometimes just sending a CMP/CBC seems so easy compared to the other stuff our patients go through. Do you have a practice to recommend for spacing labs? I know that with experience comes a much better sense of who needs to be watched more closely and who is stable, but I’ll just have to wait for that. Thanks
Hey Corey! Thanks for the question! Like you alluded to, clinical judgment driven by experience is the single most important factor. We need to tailor things based on the patient’s overall clinical picture (vital signs, physical examination, history, pre-test probabilities, etc.) In settings like the ICU, it probably does make sense to monitor labs more frequently, but in general med-surg wards, it’s hard to justify daily labs on a patient who has been stable for days and is otherwise in the hospital for a relatively minor reason.