
Complete (3°) heart block (CHB) occurs when atrial signals do not reach the ventricle; therefore, the atria (P-waves) and ventricles (wide QRS complexes) pace themselves independently of each other. Symptoms can range from fatigue and dyspnea to syncope, chest pain, and sudden cardiac death. CHB can be caused by ischemia, myocarditis (e.g. Lyme disease), endocarditis, myxedema, electrolyte derangements, and infiltrative processes (e.g., amyloidosis, malignancy, etc.). Oftentimes, no etiology is identified.
An electrocardiogram (EKG) establishes this diagnosis with treatment centered around pacing – pharmacologically with agents like atropine, epinephrine, or dopamine… or even better… transvenous pacing as a bridge to a permanent pacemaker (the definitive treatment).
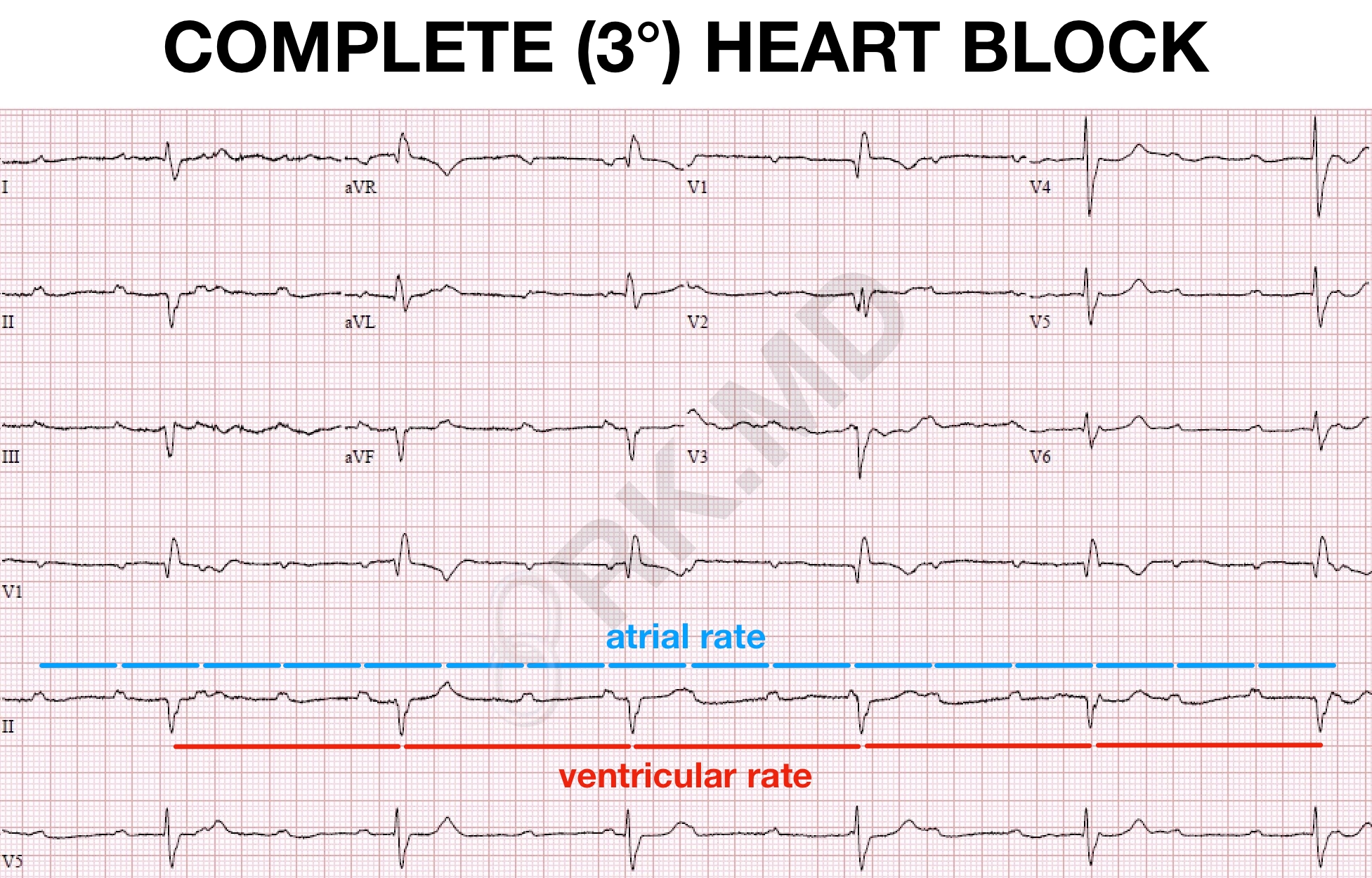
This EKG shows classic CHB with an atrial rate of ~100 bpm (blue intervals) and ventricular rate of ~35 bpm (red intervals). The ventricular escape rate and QRS morphology can provide insight into the block’s location. A ventricular rate in the 40-50s with narrow QRS suggests a block within the AV node or His bundle. A more distal block results in a slower escape rate with wide QRS.



I remember reading that atropine is mostly ineffective for 3rd degree because an intact AV node is needed.
What are your thoughts on this? I suppose there is no harm in administering atropine for CHB- is it more likely to increase the ventricular rate? or atrial rate? or? I’ve never done it personally but thats mostly because I work in a cardiac surgery ICU where pacing is 99.9% of the time a treatment option.