
Patients with bacteremia/fungemia can pose a real challenge, especially when discussing if, how, and when to exchange out existing access catheters. In other words, if I have a patient in my ICU with new gram negative rods in their blood, but they also have a port for chemotherapy and a separate tunneled central line for hemodialysis, we might have an issue removing/exchanging the aforementioned catheters in a timely and safe manner.
Instead, we are beginning to perform more catheter salvage using lock therapies with ethanol or specially concentrated formulations of antibiotics like vancomycin and ceftazidime. The idea is we inject one of the aforementioned agents into the catheter lumen, let it dwell for several hours, aspirate out the agent, saline/heparin lock the line, and repeat the procedure for multiple days. Lock therapies are to be used in conjunction with systemic antibiotics.
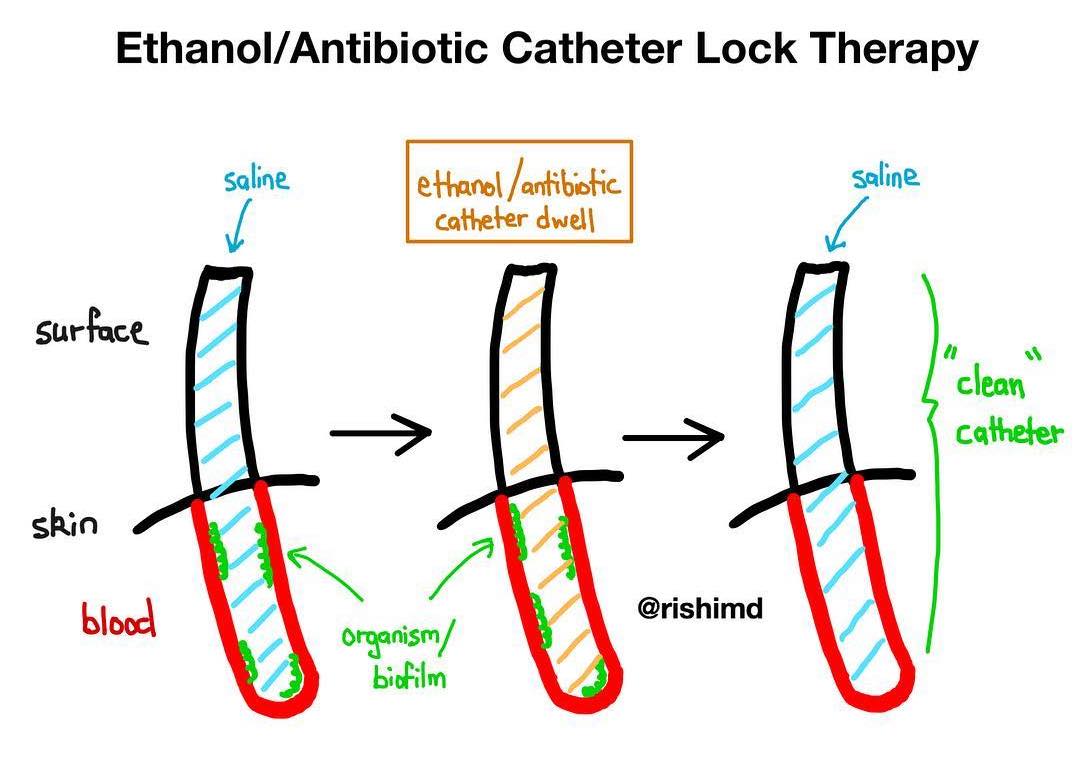
The rationale for using ethanol is that it’s a antimicrobial agent with no known clinically significant bacterial resistance. It also penetrates biofilm, a major consideration in line-associated infections. Ethanol locks are contraindicated in neonatal and pregnant patients; they should be used cautiously in patients with alcohol dependence. Additionally, ethanol locks are not recommended in hemodialysis catheters (risk of catheter degradation) or Bard brand catheters/PICCs. In these situations, consider antibiotic locks with vancomycin or ceftazidime.
Typically, I use a 70% ethanol solution and dwell for 4-12 hours/day for five days. The volume of ethanol infused into each port of the catheter varies depending on the make/model of the catheter and which specific port (proximal, distal, etc) you’re locking. Anywhere from 0.5 cc to 2 cc is required per port, but check with the manufacturer and your pharmacists!



Thanks for sharing, I was just reading about this new Mino-Lok product by Citius Pharmaceuticals that is currently in p3 trials. (p2 results were stellar, but of course small sample size) Looks like their formula is similar to yours, but not identical, (minocycline, edetate, and ethanol). https://www.citiuspharma.com/mino-lok/
Really hoping this comes through as a new therapy, it seems that it’s a much better option than remove/replace, and can (hopefully) meaningfully improve patient outcomes. Regardless of whether that happens, definitely love to see new studies and trials being conducted in this space, as it certainly seems like there is room for improvement.
Thank you so much for sharing! 🙂
So is this method only used if bacteremia is present? Or more as prophylaxis? If biofilm is on the inner surface of the catheter, can it not also be on the outer surface of the catheter? In which case a lock system will not have an effect on the other half of the biofilm having direct contact with the blood?
Excellent questions! I’ve only used this technique with known bacteremia/fungemia in high risk patients who will also be receiving systemic antibiotics/antifungals. Intuitively I don’t think there’s a good way to prove the clearance of this biofilm although we do surveillance cultures to show the resolution of the bacteremia/fungemia. *Shrug*, definitely an imperfect therapy.