
Sodium is the primary cation (positive-charged ion) in the extracellular space. Therefore, dilutional hyponatremia can occur if free water is added to the extracellular space from fluid shifts and infusions.
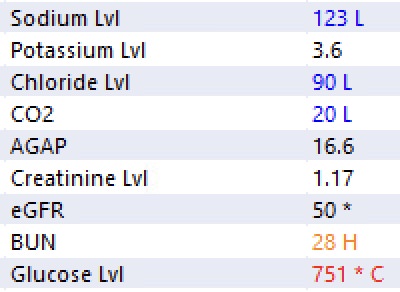
Let’s look at this basic metabolic profile. Glucose 751 mg/dL (critically high). Sodium 123 mEq/L (low). Hyponatremia is an expected finding as hyperglycemia will induce fluid shifts. Water is moved from the intracellular space to the extracellular space via osmosis.
So how do we know what the “corrected” sodium concentration is?
In 1973, MA Katz determined 1.6 to be the correction factor. In 1999, Hillier et al. challenged this (based on a study with only six patients), concluding that 2.4 was a better correction factor. In other words, for every 100 mg/dL above 100, the sodium should be increased by 2.4 mEq/L for correction. Mathematically, corrected sodium = measured sodium + 0.024 * (measured glucose – 100). In the example above, the corrected sodium is ~139 mEq/L (or normal!)
Drop me a comment below with questions!



And in this case, what is the treatment?
I don’t give out specific medical advice, but the goal will be centered around correcting and identifying the cause of hyperglycemia.