
The right ventricle (RV) is designed to be a compliant volume chamber that pumps against a low-pressure, low-resistance pulmonary arterial (PA) system. RV-PA coupling refers to the proportional alignment between RV contractility and afterload. In situations of increased RV afterload like pulmonary hypertension, the RV can adapt (e.g., anatomic remodeling such as hypertrophy) to maintain RV-PA coupling by increasing contractility to preserve RV stroke volume. However, when the RV can no longer match its contractility to increased afterload, RV-PA uncoupling occurs, leading to RV dysfunction, decreased stroke work (SW), and clinical right heart failure.
RV-PA coupling is mathematically defined as the RV end-systolic elastance (Ees, a load-independent surrogate for contractility) divided by the effective PA elastance (Ea, a pulsatile component in addition to steady components like PVR and mPAP). In other words, it’s the RV’s performance divided by the afterload imposed on the RV. An Ees/Ea ratio of 1.5 – 2.0 represents RV-PA coupling at an ideal balance of RV work and oxygen consumption. With echocardiography, RV-PA coupling can be estimated with TAPSE/PASP where ~1.2 is normal, and mortality is increased if < 0.64 mm/mmHg.
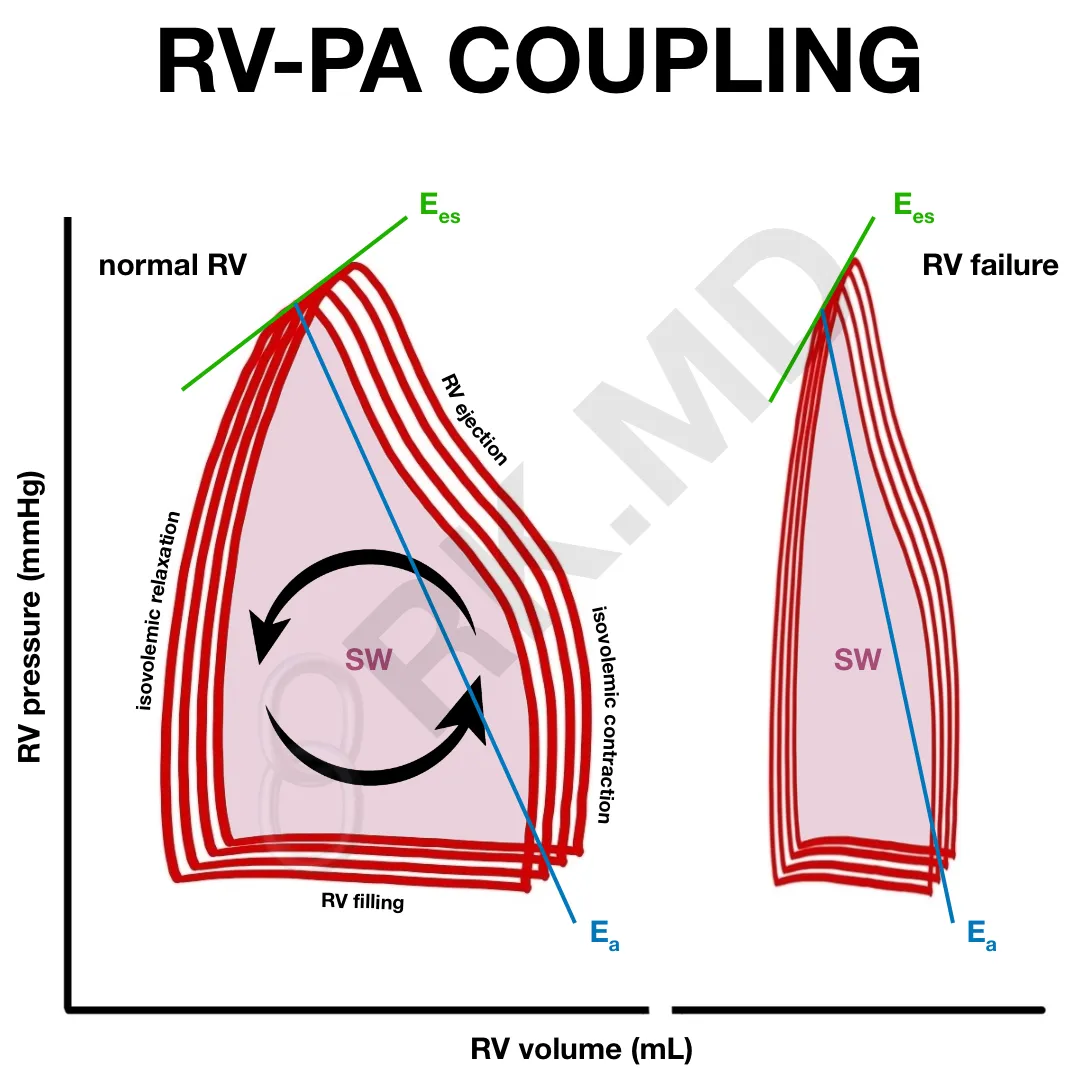
Multibeat pressure-volume (PV) loops with varying preloads can be used to determine the elastance values where Ees is the slope through the end-systolic pressures (green line), and Ea is estimated by the end-systolic pressure and stroke volume (blue line). Newer approaches use strain echocardiography and pulse wave velocities to determine the extent of (un)coupling.
Drop me a comment with questions!



Thank you 🙏
You’re welcome!
Amazing
Thank you! 🙂